
The Neurology of Masked Symptoms In advanced neurodegeneration, the brain often fails to correctly process or communicate localized pain signals. Instead of telling a carer that it hurts to urinate, a resident’s body reacts to the internal physiological stress. This manifests not as a physical complaint, but as a sudden, sharp shift in baseline behaviour.
Key Atypical Triggers Your Team Must Watch For:
Acute Cognitive Decompensation: A sudden, catastrophic drop in cognitive baseline (different from the gradual decline of dementia) usually points to an underlying physical infection or delirium.
Paradoxical Agitation or Lethargy: A resident who is typically calm suddenly becoming highly aggressive, or conversely, an active resident becoming profoundly lethargic and refusing food.
Sudden Incontinence or Mobility Changes: A sudden spike in unexplained falls or a new onset of urinary incontinence in a previously continent resident is a classic red flag.
Beyond the Physical:
Spotting Atypical UTI Presentations in Complex Dementia
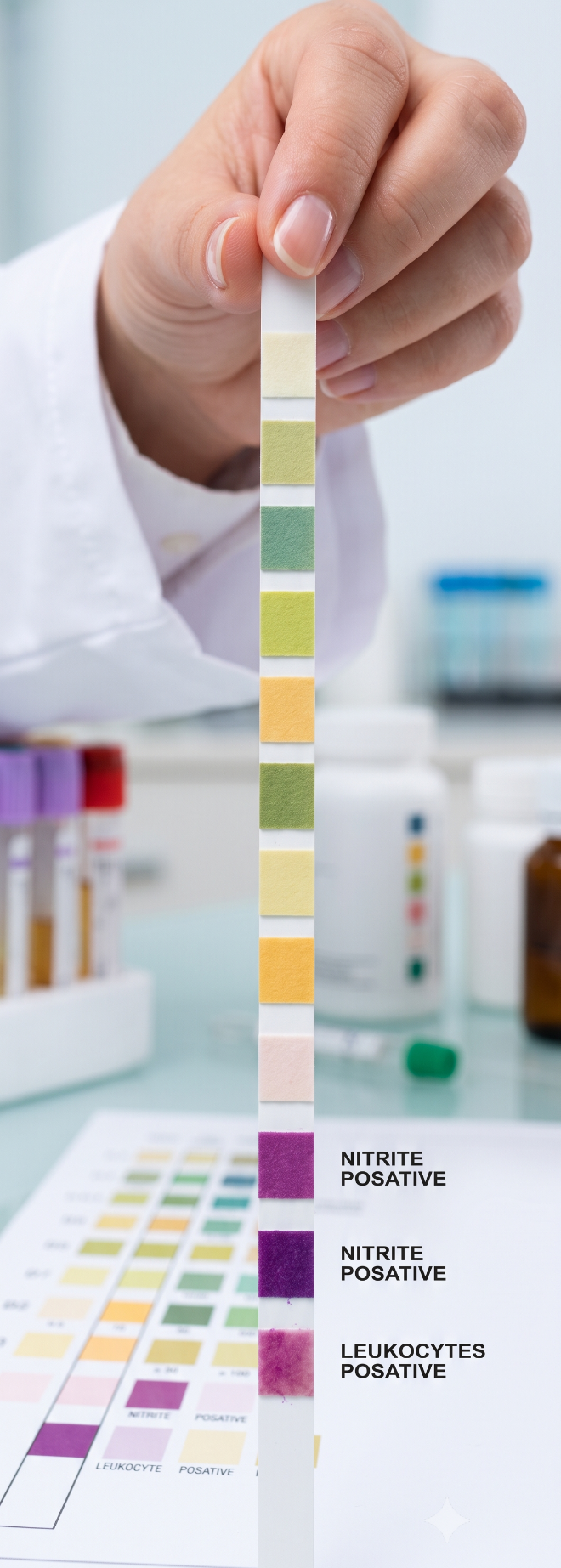
Moving Past the Dipstick Dip-CQC Compliance Relying solely on reagent dipsticks in the elderly population often leads to over-prescribing due to asymptomatic bacteriuria. Clinical governance demands a holistic assessment.
To safeguard your residents and reduce avoidable hospital admissions, care teams must be trained to utilise robust clinical frameworks. Training your staff to document these subtle behavioural shifts accurately means you can present high-quality, objective evidence to visiting GPs, ensuring swift, accurate targeted treatment.
Below are some examples of frameworks commonly used in residential care settings to monitor, diagnose or prevent UTIs in their residents:
For nursing home managers and clinical leads, Urinary Tract Infections (UTIs) are a constant clinical battleground. However, in residents living with advanced, non-verbal dementia, relying on classic diagnostic symptoms like dysuria, frequency, or fever is a recipe for missed diagnoses. By the time a physical symptom becomes glaringly obvious, the resident may already be spiralling toward acute delirium, a severe fall, or sepsis.
As a clinical educator, one of the most vital skills I train care teams to develop is the ability to read behavioral changes as acute clinical indicators.
1. The "To Dip or Not to Dip" Pathway
This is the most widely adopted quality improvement framework across UK care networks. Its primary purpose is to completely stop the standard practice of routine urine dipstick testing for residents over 65, which often yields false positives due to harmless background bacteria. Instead, care home staff use a strict clinical flowchart. A suspected UTI is only tracked or escalated if a resident shows a new onset of painful urination alone, or two or more specific clinical symptoms, such as new incontinence, worsening confusion, or a high fever.
2. The TARGET UTI Care Home Assessment Tool
Developed by national public health agencies, this structured tool is a mainstay for front-line communication. It acts as a standardized checklist and communication passport between the nursing home and the GP. The care home nurse completes a form covering four distinct areas: excluding other infection sources (like chest infections), identifying specific new urinary symptoms, checking for physiological red flags (like rapid heart rate), and assessing localized pain. This form ensures objective tracking and clinical justification before antibiotics are prescribed.
3. SBAR (Situation, Background, Assessment, Recommendation)
While not exclusive to UTIs, SBAR is the universal clinical communication tool mandated across healthcare and social care settings to track acute resident deterioration. It prevents vague reporting by forcing a structured, evidence-based overview of a resident's condition. When a UTI is suspected, a nurse uses a specific UTI-SBAR template to document the precise clinical timeline, baseline vital signs, and specific changes in the resident's behaviour or urine characteristics before contacting medical professionals.
4. Regional "Days Since Last UTI" Trackers
Many regional health boards provide care homes with continuous dashboard trackers. Rather than just diagnosing an individual, these tools track the care home’s wider environment. They log continuous data on hydration initiatives, catheter care audits, and the total number of days the facility has gone without a healthcare-associated infection. This shifts the focus from reactive treatment to proactive prevention across the entire care home.
Managing UTIs in advanced dementia is not about waiting for a physical symptom to appear; it is about building a culture of proactive, structured vigilance. When care teams are trained to view acute behavioural shifts as urgent clinical data, the entire dynamic of care changes. We move away from the reactive, often dangerous reliance on urine dipsticks and toward an evidence-based approach that satisfies both clinical governance and Care Quality Commission (CQC) expectations.
Implementing structured frameworks like the "To Dip or Not to Dip" pathway or the TARGET assessment tool does more than just streamline GP communication. It empowers your front-line care assistants—the people who know the residents best—to become the ultimate defenders against silent infections. By capturing subtle changes early and documenting them objectively, you can confidently halt clinical deterioration long before it triggers a crisis, a fall, or an avoidable hospital admission.
As a clinical leader, the challenge is to embed these frameworks into daily handover routines. Review your tracking systems, audit your team’s communication methods, and ensure that "a change in baseline behaviour" is always met with a rigorous, holistic assessment. In the battle against silent infections, structured data is your most powerful medicine.